Support the Prepare Act
Public Health Reinvestment and Emergency Pandemic Adaptability, Readiness and Efficiency
Introduction
The public health system in New York State is in crisis. Numerous elements have conspired to weaken our public health response infrastructure to a point of unprecedented fragility due to ten consecutive years of disinvestment by the state; a malignant and ongoing loss of public health workers; a demoralized public health system diminished by inadequately supported workload demands; the ongoing response to the covid pandemic; and the specter of an anticipated wave of public health staff retirements that will further diminish our public health response and prevention capabilities.
We are at what is perhaps the most meaningful public health inflection point in our lifetime, where only sound policy and resource decisions will steer us back to a path that will ensure our public health system is prepared for even greater challenges that we know will come.
In short, your leadership and support has never been needed more to protect the lives and health of the people of New York.
Within this confluence of factors, however, we see opportunity. The public better understands the real and deadly impact of public health threats, and the immeasurable value of a fully prepared public health system; our governor understands and honors the value of local partners, and the value of partnership and collaboration with the Legislature; and historic levels of state resources are available as we enter the coming budget season.
For the first time in decades, we fully comprehend the value and the needs of our public health system, and at the same time possess the financial means and public support to effectively address these needs.
These factors align to beg a simple question: If not now, then when?
The answer is clear. It must be now.
Background on Article 6 State Aid Funding
Article 6 of the Public Health Law provides statutory authority for state aid for general public health work. The program provides reimbursement for expenses incurred by local health departments (LHDs) for core public health areas as defined in law. For more information on article 6, please read page 7-9 of NYSACHO’s budget testimony document.
Why Support the PREPARE Act?
New York State’s local public health workforce is responsible for promoting and protecting the health of New York’s communities. Working for one of New York State’s 58 local health departments, the local public health workforce – made up of public health nurses, disease control investigators, sanitarians, community health workers and other professionals – is responsible for preventing disease, protecting the health of New Yorkers, and keeping our communities safe.
Most of the staff in the state’s local health departments (LHDs) work to deliver one or more of six core public health services: community health assessment, communicable disease control, chronic disease prevention, maternal and child health services, emergency preparedness services and in 31 of the 58 local health departments, environmental health services. These six core responsibilities are set forth in statute and are known as Article 6 services as they are reimbursed by the state through the statutory mechanisms authorized in Article 6 of the public health law. The six cores, or basic, services provide the minimum foundational public health responsibilities delivered by local health departments; however, additional statutory and programmatic mandates fall under these six broad service areas.
Unfortunately, over the past five years in New York State, the number of LHD staff delivering Article 6 core services has declined. According to data from the New York State Department of Health, the number of FTEs working on Article 6 services declined by 7% between 2015 and 2020. During this same period, the population of the state increased by 3%. This reduction in staff has made it harder for the state’s local health departments to address the public health challenges facing their communities, including responding to the COVID-19 pandemic. While the largest reduction in staff was experienced by the New York City Department of Health and Mental Hygiene, other LHDs also experienced a decline.

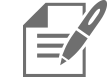
 In fact, most of New York’s LHDs do not have sufficient staff needed to provide a basic package of public health services. According to the Public Health Center for Innovations and the de Beaumont Foundation, local health departments nationally need approximately 54,000 new staff to be able to provide adequate infrastructure and a minimum package of public health services. When applying this formula for how many local public health workers each community needs to New York’s LHDs, an estimate showed that 90% of LHDs do not have enough staff to adequately provide basic foundational public health services to their communities. In total, over 1,000 additional Full-Time staff are needed to be able to provide an adequate infrastructure and a minimum package of public health services.
In fact, most of New York’s LHDs do not have sufficient staff needed to provide a basic package of public health services. According to the Public Health Center for Innovations and the de Beaumont Foundation, local health departments nationally need approximately 54,000 new staff to be able to provide adequate infrastructure and a minimum package of public health services. When applying this formula for how many local public health workers each community needs to New York’s LHDs, an estimate showed that 90% of LHDs do not have enough staff to adequately provide basic foundational public health services to their communities. In total, over 1,000 additional Full-Time staff are needed to be able to provide an adequate infrastructure and a minimum package of public health services.
Leaving public health underfunded will result in even more illness and death and place an even greater strain on state and local resources as they try to fill the gaps left in these essential services. For more information on the function of local health departments in New York State.
Public Health Burnout and the Experiences of Public Health Workers
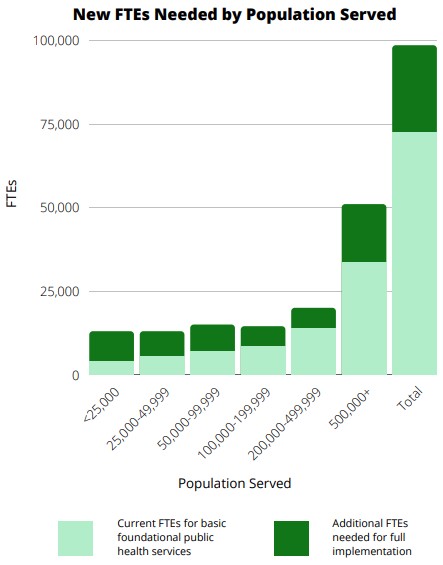
 According to a survey led by SUNY Oneonta, Bassett Healthcare Network Research Institute and the New York State Association of County Health Officials, Pain and Perseverance, public health workers have been subject to targets of protests and have experienced overwhelming burnout while responding to the pandemic. Of the two-hundred and nine public health workers who completed the survey, data indicates:
According to a survey led by SUNY Oneonta, Bassett Healthcare Network Research Institute and the New York State Association of County Health Officials, Pain and Perseverance, public health workers have been subject to targets of protests and have experienced overwhelming burnout while responding to the pandemic. Of the two-hundred and nine public health workers who completed the survey, data indicates:
- 90.4% of respondents have felt overwhelmed by workload.
- 75.6% felt disconnected from family and friends because of workload.
- 65% felt unappreciated at work and 75% felt inadequately compensated.
- Over half of respondents reported experiencing stigma or discrimination during the crisis.
- 35% received job-related threats because of work by members of the public.
- 55% felt bullied or harassed because of work by the members of the public.
- 30% have received any sort of hate mail/email/messages from the public.
 To protect and retain the dedicated workers employed by local health departments, investments need to be made to article 6 state aid funding to ensure that these public health entities are appropriately staffed and thus able to allow employees to manage work-life balance and avoid burnout. Making such investments will protect and ensure longevity in the state’s public health workforce. Despite all this, local health departments have stood up to the challenges faced to address the pandemic all the while vaccinating tens of thousands of New Yorkers and continue to do so as we face a possible third surge this winter.
To protect and retain the dedicated workers employed by local health departments, investments need to be made to article 6 state aid funding to ensure that these public health entities are appropriately staffed and thus able to allow employees to manage work-life balance and avoid burnout. Making such investments will protect and ensure longevity in the state’s public health workforce. Despite all this, local health departments have stood up to the challenges faced to address the pandemic all the while vaccinating tens of thousands of New Yorkers and continue to do so as we face a possible third surge this winter.New York’s Looming Public Health Workforce Retirement Crisis
 Based on a survey conducted by NYSACHO, the state is approaching the loss of decades upon decades of public health expertise through local retirements. It is only a matter of time before a large segment of the public health workforce begins to retire and we need to be realistically prepared to rebuild the public health system when we are confronted with another public health crisis. Retirement survey findings indicate:
Based on a survey conducted by NYSACHO, the state is approaching the loss of decades upon decades of public health expertise through local retirements. It is only a matter of time before a large segment of the public health workforce begins to retire and we need to be realistically prepared to rebuild the public health system when we are confronted with another public health crisis. Retirement survey findings indicate:
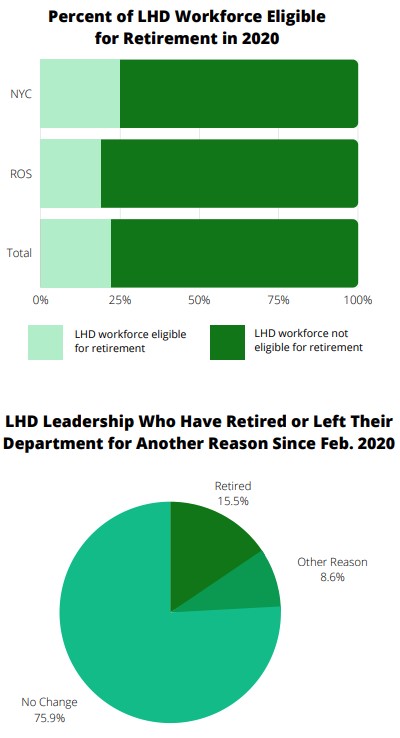
- 42 LHD respondents reported a total of 1257 LHD employees statewide were eligible to retire in 2020.
- Of these, 743 were in NYC and 514 in rest of state. This represents a total of 22% of the LHD workforce statewide who were eligible for retirement in 2020, with 25% of the NYC LHD workforce eligible to retire, and 19% of the total LHD workforce outside of NYC eligible to retire.
- Out of 45 LHDs responding, 23 indicated that they had employees who intended to retire in 2021, for a total of 69 employees statewide.
- The decade plus of disinvestment and erosion in public health has left little opportunity for succession planning and development of the next generation of public health professionals. Additionally, shortages in fields such as nursing and engineering have resulted in longer periods for recruitment to fill vacancies, as well as competition from the private sector that impacts employee retention. Local governments will be hard pressed to address the convergence of looming retirements and profession shortages under the current funding structure.
- Out of 43 LHDs respondents, 33 indicated that they had employees who had, or intended to retire by the end of 2020, for a total of 236 employees statewide.
- Since the start of the COVID-19 pandemic, New York has seen 9 out of 58 local health officials (leadership positions within health department) retire and 5 county health officials leave for other/unidentified reasons.
The decade plus of disinvestment and erosion in public health has left little opportunity for succession planning and development of the next generation of public health professionals. Additionally, shortages in fields such as nursing and engineering have resulted in longer periods for recruitment to fill vacancies, as well as competition from the private sector that impacts employee retention. Local governments will be hard pressed to address the convergence of looming retirements and profession shortages under the current funding structure.
Medical Examiner/Coroner Services: Lack of State Support for Vital Death Investigations
Death investigations are a critical public health activity. While the popular view of these services focuses on investigations related to criminal activity, under New York state statute, coroners or medical examiners have jurisdiction and authority to investigate every death within their county, or body found within the county, which is or appears to be:
- A violent death, whether by criminal violence, suicide or casualty;
- A death caused by unlawful act or criminal neglect;
- A death occurring in a suspicious, unusual or unexplained manner;
- A death caused by suspected criminal abortion;
- A death while unattended by a physician, where no physician is able to certify the cause of death.
- A death of a person confined in a public institution other than a hospital, infirmary or nursing home (i.e. in a jail).
In addition to deaths related to criminal activity, commonly encountered reportable unnatural deaths include:
- Opioid related deaths.
- Deaths where a motor vehicle was involved.
- Infectious deaths following an injury.
- Hip fractures in the elderly.
- Deaths where either the result or contributory cause was due to subdural hematoma.
- Any death by asphyxiation.
- Head injuries with a prolonged hospital course.
- Cases where there is uncertainty or inadequate clinical information at the time of admission or death.
- Cases transferred from out of the county where there may be inadequate information.
- Deaths from conditions directly related to trauma regardless of the passage of time – e.g. death from a seizure disorder that was the result of a motor vehicle accident, a fall, or being struck on the head.
Many medical examiners offices also provide pathology and toxicology services to counties served by coroners. In 2019, the 20 counties operating medical examiner programs accounted for roughly $108M of the $122M or roughly 88.5% of the total 2018 budget for coroner and medical examiner services across all of the counties in NYS.
Prior to 2011, county coroners and medical examiners were recognized as a core public health service, with medical examiner services reimbursed up to 36 percent with state aid from Article 6 funding to local health departments.
In 2011, the State Budget recommended shifting the reimbursement for medical examiners from the New York State Department of Health (NYSDOH) to the New York State Department of Criminal Justice Services (DCJS). County objections over the need for objectivity and distance from criminal justice agencies were recognized as a valid concern, however, rather than returning funding to Article Six reimbursement, the funding simply was no longer available as the state continued to deem this activity to be a public safety and not a public health function.
Since that loss of state support for ME services, the public health need for these services has grown. Death investigations and data are a critical piece in addressing the ongoing Opioid epidemic, particularly as many opioid-related deaths are unattended. Similarly, toxicology results help identify new trends in street drugs, such as the rise in drugs mixed with fentanyl. A key part of the COVID-19 response, particularly in the early time period of the epidemic, was equally critical to informing disease incidence, contributing health factors for COVID deaths, as well as death rates.
The Governor and State lawmakers must restore funding to counties to help offset the increasing costs for state-mandated autopsy services in recognition of the critical public health data provided by death investigations. Given the 2011 loss of funding, and subsequent increases in costs and challenges facing county coroner and medical examiner services, NYSACHO joins the New York State Association of Counties (NYSAC) and the New York State Association of County Coroners and Medical Examiners (NYSACCME) to request that the state to fund 50 percent of the autopsy and toxicology services impacting counties due to the changing pathology landscape in NYS and the opioid epidemic.
Fully Fund the Implementation of the 2019 Elevated Blood Lead Level Mandate
 Lead Poisoning Prevention Activities delivered by local health departments are supported through a variety of funding mechanisms, including the Lead Poisoning Prevention Program, Childhood Lead Poisoning Primary Prevention Program (15 counties), Healthy Neighborhood Program (some counties), and reimbursement through Article Six Public Health Law General Public Health Work funding.
Lead Poisoning Prevention Activities delivered by local health departments are supported through a variety of funding mechanisms, including the Lead Poisoning Prevention Program, Childhood Lead Poisoning Primary Prevention Program (15 counties), Healthy Neighborhood Program (some counties), and reimbursement through Article Six Public Health Law General Public Health Work funding.
When the definition of elevated blood lead level (EBLL) was lowered to 5 ug/dL or greater, the state also allocated an additional $9.7 million to Article Six state aid. This investment falls short of the $30.3 million in funding needed and places the majority of the cost burden on the local tax levy, including 100% of fringe costs associated with any new staff hired to provide public health interventions and case management for the additional children requiring services. This estimated need is based on an average cost per case of nursing case management of $713 and an average cost of $2123 per case for environmental management activities.
We recommend that all monies allocated for funding the expanded mandate (current and future) be appropriated into the Lead Poisoning Prevention program of the New York State Department of Health. We further recommend that this funding then be distributed to the local health departments through existing grant mechanisms to support implementation of the expanded mandate. Allocating existing and new investments to support the lower EBLL through this program will allow local health departments to secure and maintain the necessary staffing and other resources required accomplish the goals set forth by the state mandate, whilst ensuring that New York State keeps its promise to property taxpayers through its enactment of a permanent property tax cap.
Solutions: Investing in New York’s Public Health Infrastructure
 Public health work, particularly response to emergencies like the COVID-19 pandemic, requires trained, highly educated workforce. New York State sets minimum qualifications for 13 public health titles; all but one of these requires a minimum of a bachelor’s degree and several require advanced degrees. Given other employment opportunities and the typically lower salary rates of public vs. private sector jobs, fringe benefits are critical for recruitment and retention of a qualified, experienced workforce. Provision of the core public health services required by New York State under Article Six requires that LHDs maintain this educated and highly trained workforce.
Public health work, particularly response to emergencies like the COVID-19 pandemic, requires trained, highly educated workforce. New York State sets minimum qualifications for 13 public health titles; all but one of these requires a minimum of a bachelor’s degree and several require advanced degrees. Given other employment opportunities and the typically lower salary rates of public vs. private sector jobs, fringe benefits are critical for recruitment and retention of a qualified, experienced workforce. Provision of the core public health services required by New York State under Article Six requires that LHDs maintain this educated and highly trained workforce.
Emergency funding for public health threats does not sustain workforce investment. LHDs cannot retain and utilize experienced staff hired for emergency response when funding is time limited. Skills needed and core services provided during COVID-19 and other public health emergencies are those that are used every day for core public health services.
 The current fringe ineligibility set forth under Article 6 does not work efficiently in a post clinical care public health model. When Article Six was initially enacted, clinical care revenues reduced, or often fully covered fringe expenses; at that time, localities were the safety net providers of primary and clinical home care services in a fee-for-service payment model, to provide basic care for un- and under-insured populations. New payment models and expansion of the availability of health care meant that LHDs were largely no longer needed as safety net providers. Rather than reinvesting public health dollars from clinical care to population health services, public health funding was simply reduced. Concurrently, while the state disinvested in existing population health services and expertise provided by local health departments, it directed funding towards pushing clinical care providers towards population health services; rather than coordinating the two, too often, clinical care simply duplicated public health services. COVID-19 showed why clinical care and public health have unique and complementary roles to play, with clinical care focused on individual health and public health focused on population health.
The current fringe ineligibility set forth under Article 6 does not work efficiently in a post clinical care public health model. When Article Six was initially enacted, clinical care revenues reduced, or often fully covered fringe expenses; at that time, localities were the safety net providers of primary and clinical home care services in a fee-for-service payment model, to provide basic care for un- and under-insured populations. New payment models and expansion of the availability of health care meant that LHDs were largely no longer needed as safety net providers. Rather than reinvesting public health dollars from clinical care to population health services, public health funding was simply reduced. Concurrently, while the state disinvested in existing population health services and expertise provided by local health departments, it directed funding towards pushing clinical care providers towards population health services; rather than coordinating the two, too often, clinical care simply duplicated public health services. COVID-19 showed why clinical care and public health have unique and complementary roles to play, with clinical care focused on individual health and public health focused on population health.
In addition to these structural issues with state aid for general public health work, further disinvestments at the state level during this time period included cost shifts, such as the elimination of any state support for medical examiner services, and un- and under-funded new or expanded mandates through both statute and regulation. Examples include the lowering of the actionable blood lead level, or the monitoring of cooling towers for legionella, which added significant workload with little to no resources to carry out that work. Requiring a more thorough assessment of both the state and local fiscal impact of public health policy changes in advance of their adoption can assure that important public health policy goals are fully realized in their implementation.
Components of the New York State PREPARE Act
The public health reinvestment and emergency pandemic adaptability, readiness, and efficiency (PREPARE) act is designed to increase the infrastructural state funding supporting local health departments’ provision of the core public health services needed to provide a base level of protection to the communities they serve. State reinvestment in the funding for local health departments will help retain and sustain a responsive, skilled public health workforce necessary to take prompt action in public health emergencies. Over the past decade, the local public health workforce has decreased by one-third while public health emergencies have been increasing.
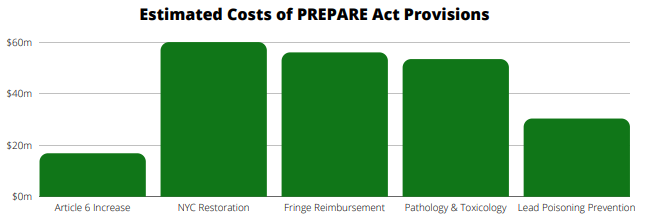
- Increase Article 6 base grant for full service LHDs (37) to $750,000 or $1.50 per capita. Total increase over current base grant= $15.19 million
- Increase Article 6 base grant for partial service LHDs (21) to $577,500. Total increase over current base grant=$1.62 million
- Restore NYC to 36% reimbursement beyond the base grant under Article 6 state aid. Total cost NYC restoration=$60 million annually
- Permit fringe benefits as an eligible expense under article 6 state aid and reimburse fringe at 36% in all counties. Total estimated cost of fringe reimbursement at 36%=$56 million
- Provide state reimbursement of 50% for pathology and toxicology services provided by county medical examiners. Total estimated cost=$53.4 million (based on 2018 budgets)
- Fully fund the implementation of the 2019 Elevated Blood Lead Level Mandate. Total estimated cost=$30.3 million
Conclusion
These asks are not insignificant sums of money; however, they represent both the needs for basic infrastructure to deliver core public health services and the current burden that rests on local property payers. The County Health Officials of New York and their association, NYSACHO, look forward to working with you to develop the policies and identify the resources and services necessary to rebuild New York’s public health infrastructure. If not now, then when?
The New York State PREPARE Act
Public Health Professionals serve as both a safety net and first responders against population health threats.
Reinvestment is the right thing to do. COVID-19 revealed both the strength and the fragility of our public health system. Investing long-term in public health assures that the highly trained and skilled workforce is available when a crisis occurs.
Emergencies and pandemics are not extraordinary events in public health. While the COVID-19 pandemic has been characterized as unprecedented, it is not the first pandemic in this century, not the first emerging public health threat; it is merely exceptional in its scope. Whether it is H1N1, Ebola, Zika, COVID-19 or emerging contaminants in drinking water, the truth is that public health emergencies can, and do, occur frequently. Public health workers respond to emergencies, regardless of scale, every year.
Adaptability is a cornerstone of public health. During COVID-19, local health departments adapted their pandemic response, tracking, implementing, or monitoring 122 Executive orders and close to 500 guidance documents. In the United States alone, there have been 10 SARS CoV-2 variants monitored, including the Delta variant which resulted in changes in response for vaccinated individuals. Similarly, the availability of vaccine and processes for distribution have evolved as supply has expanded and new groups have become eligible. And COVID-19 disease and vaccine misinformation has required local health departments to continually monitor and adapt messaging to assure that science-based, accurate information is communicated with the public.
Readiness is the hallmark of public health. Many disease threats require immediate and swift public health responses. Similarly, other emergencies, such as weather events or harmful algal blooms, require rapid action to reduce the threat of illness, injury, and loss of life. It is through their daily work and ongoing emergency preparedness drills and response that the public health workforce assures a high-level of readiness for emergency events.
Efficiency in funding is needed to provide optimal stewardship of public resources. The continued pattern at the state and federal level of providing short-term, time limited funding for specific public health emergencies does not allow local health departments to develop and maintain the highly trained workforce necessary for response. Just-in-time training and reliance on volunteers does not provide continuity of response, nor does it allow ongoing system improvements through drills, exercises and every-day public health activities that are the cornerstone of a strong public health infrastructure.
Make it Personal! If you want to share how the policy impacts you, please feel free to use our text as a starting point to draft a message to send directly to your representatives. Click here to Find Your NYS Assembly member(s), or here to find your NYS Senator(s).